
May 2026

Yearly Reminders
Cancer Screenings
Breast Cancer
Screen yearly with a mammogram for women aged 40-75. Gender diverse folk with breasts, please get in touch with Dr. Neuman for a case-by-case scenario.
Cervical Cancer
Screen every three years with a pap smear for women (or anyone with a cervix) aged 21 to 29, and every five years with a pap smear + HPV testing or HPV testing alone for women aged 30-65.
Colon Cancer
Screen every 10 years with a colonoscopy for folks 45 to 75. Most folks without family history or personal history of colon cancer or advanced polyps can substitute colonoscopy for the Cologuard stool test every 3 years or stool testing every year.
Lung Cancer
Screen yearly with a low-dose CT Scan for current or past smokers with a history of 20+ years of 1 pack/day smoking, aged 50-80
Prostate Cancer
Screen yearly with a PSA blood test on a case-by-case basis for those 40+ with high risk, or 50+ with standard risk
Other Cancers
Depends on individual risk, but typically, they are not screened for because there is insufficient evidence that the benefits outweigh the harms for the average-risk person.
Vaccines
RSV
For everyone age 50+ and those younger at higher risk, one time.
TDap
For everyone, every 10 years.
Pneumonia
For everyone age 65+ and those younger at higher risk, one time, or every five years for folks at high risk.
Flu
For everyone, yearly.
COVID
For everyone, yearly.
HPV vaccine
For everyone before age 27, for those sexually active with new partners age 27+, one dose is great, a three-part series is best.
Shingles
For everyone age 50+, a two-dose series is recommended.
Other screening recommendations
Abdominal Aorta Aneurysm
Screen one time with an ultrasound for 65-75-year-old men who have ever smoked.
Sexually Transmitted Infections
Screen yearly with blood and urine tests for anyone at risk, including anyone sexually active, particularly with a history or current multiple partners.
HepatitisC
Screen one time with a blood test for all adults.
High Blood Pressure, High Cholesterol, and Diabetes
Screening yearly with blood tests and blood pressure measuring for all adults 35+ or anyone younger if overweight or inactive.
Osteoporosis(weak bone/risk of fracture)
Screen with DEXA bone scan every 2-10 years for women 65+ or others at high risk of fracture.
General Recommendations
9 fruits/veggies servings daily.
150 minutes of moderate exercise or 90 minutes of intense exercise weekly.
7-9 hours of sleep.
Twice-yearly dental cleaning.

Do you still need that medication?
Deprescribing is the practice of stopping a medication that is no longer needed, or that may be doing more harm than good. A new study provides a prime example of why deprescribing can be beneficial. Many people were started on low doses of levothyroxine (Synthroid) years ago based on older guidelines. Since then, research has shown that thyroid hormone levels naturally shift with age. Guidelines have been updated to reflect this, but many people, particularly older adults, are still taking levothyroxine based on the original standards.
This new study looked at 370 adults aged 60 and older. Half of the participants discontinued levothyroxine per updated guidelines, which recommend discontinuation when TSH (thyroid-stimulating hormone, the primary test used to measure thyroid levels) is below 10. Among those who had been taking 50 mcg or less, 63% successfully stopped the medication, with no change in quality of life and thyroid levels remaining within the updated normal range. Among those taking 75 mcg or less, the success rate was 45%. The success rate of discontinuation was much lower for folks taking over 100 mcg a day.
Dr. Neuman says: "For patients taking less than 100 mcg of thyroid replacement hormone who are interested in reducing or stopping their dose, I will now routinely suggest considering a discontinuation trial. I find it valuable to periodically ask whether any treatment we started for a good reason is still the right fit: whether the support is needed still, or whether it's become too much, too little, or no longer necessary at all."
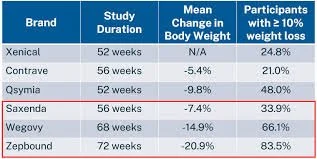
GLP-1s Updates
It's been a busy month in the world of GLP-1 medications. Here's what's new:
Wegovy HD (high-dose semaglutide) is now available: a version of Wegovy that is three times the prior maximum dose (7.2 mg weekly vs 2.4 mg weekly).
Wegovy (semaglutide) pill price drop: through NovoCare direct pharmacy, the starting dose of 1.5 mg daily is now $150 a month, and the top dose of 25 mg daily is $300 a month.
Foundayo (orforglipron) is now available: the latest GLP-1 to hit the market, Eli Lilly's orforglipron is comparably priced to existing competition Wegovy/Rybelsus (semaglutide) pills. Foundayo can be taken with or without food, unlike oral semaglutide, which is best absorbed when taken on an empty stomach. Foundayo has significantly more drug-drug interactions (including grapefruit) than the semaglutide pill versions.
Two new safety studies were published: one showing that more muscle is lost than previously suspected, and another showing a loss of heart-protective effects when stopping GLP-1s.
Dr. Neuman says: "Medicine has entered a strange, exciting, and unnerving fever dream: peptides, AI medbots, and genomic Medicine. What a trip it has all been recently."
New Med for Stroke Prevention
Asundexian, a new type of medication that blocks part of the clotting pathway (a Factor XIa inhibitor), has just cleared phase III trials. It reduced the risk of repeated stroke by 26%, from an overall risk of 8.4% to 6.2% per year, in people who have already had strokes. Importantly, it showed these improvements without an increased risk of bleeding or side effects compared to placebo.
Dr. Neuman says: "A breakthrough without apparent large risks. With these results, it is expected to obtain FDA clearance without issue, as they have already started reviewing through their Fast Pass system. It could still take up to a year or more before it is on pharmacy shelves."
A Much Needed Addiction Med
We have medicines that help people stop or reduce nicotine, like varenicline (Chantix), which increases the chances of quitting nicotine by a factor of three, and bupropion (Wellbutrin). We also have medicines for opioids (heroin or pain pills) like buprenorphine (Suboxone) and methadone, and medicines for alcohol, like naltrexone (Vivitrol) and disulfram (Antabuse). Until recently, no medication has been proven to work better than a placebo for people trying to stop or reduce methamphetamines.
A new study found that people taking mirtazapine took meth on significantly fewer days compared to those taking a placebo: 7 days vs 28 days over 12 weeks.
Dr. Neuman says: "These results are particularly exciting because mirtazapine is a safe, well-tolerated medication already routinely used to help folks with getting to sleep, depression, and increasing appetite. We don't have data yet on whether mirtazapine will work for those struggling with structurally similar compounds to meth, like cocaine or prescription stimulants; I'm hoping this study will fuel more research into helping those who are having trouble quitting or reducing."